What Are the Goals of Care When Working With Families According to the Family Health System?
Caring for Families
Objectives
Cardinal Terms
Family unit, p. 116
Family as context, p. 121
Family as patient, p. 121
Family equally system, p. 122
Family caregiving, p. 126
Family forms, p. 117
Hardiness, p. 121
Reciprocity, p. 127
Resiliency, p. 121

evolve.elsevier.com/Potter/fundamentals/
The Family
The family is a central establishment in American society; however, the concept, structure, and functioning of the family unit unit continue to alter over time. Families face many challenges, including the effects of health and illness, childbearing and childrearing, changes in family structure and dynamics, and caring for older parents. Family unit characteristics or attributes such as immovability, resiliency, and diversity help families adapt to challenges.
Family unit immovability is the term for the intrafamilial system of support and structure that extends beyond the walls of the household. For example, the parents may remarry or the children may leave home every bit adults, but in the end the "family" transcends long periods and inevitable lifestyle changes.
Family resiliency is the power of the family to cope with expected and unexpected stressors. The family unit's ability to arrange to function and structural changes, developmental milestones, and crises shows resilience. For example, a family is resilient when the wage earner loses a job and some other fellow member of the family takes on that role. The family survives and thrives as a result of the challenges they encounter from stressors.
Family diversity is the uniqueness of each family unit of measurement. For example, some families experience union for the commencement time and so accept children in subsequently life. Another family may include parents with immature children also as grandparents living in the home. Every person within a family unit unit of measurement has specific needs, strengths, and of import developmental considerations.
As you care for patients and their families, you are responsible for understanding family dynamics, which include the family makeup (configuration), construction, function, problem-solving, and coping capacity. Apply this knowledge to build on the family's relative strengths and resources (Duhamel, 2010). The goal of family-centered nursing care is to promote, back up, and provide for the well-being and health of the family unit and private family members (Astedt-Kurki et al., 2002; Joronen and Astedt-Kurki, 2005).
Concept of Family unit
The term family unit brings to mind a visual image of adults and children living together in a satisfying, harmonious manner (Fig. x-i). For some this term has the contrary prototype. Families stand for more than a set of individuals, and a family is more than a sum of its private members (Kaakinen et al., 2010). Families are as diverse equally the individuals who compose them. Patients have deeply ingrained values about their families that deserve respect. You lot demand to understand how your patients define their family. Think of the family as a gear up of relationships that the patient identifies equally family or every bit a network of individuals who influence 1 another'southward lives, whether or non at that place are actual biological or legal ties.
Definition: What Is a Family?
Defining family initially appears to exist a simple undertaking. Nevertheless, dissimilar definitions outcome in heated debates amidst social scientists and legislators. The definition of family is significant and affects who is included on health insurance policies, who has access to children's school records, who files joint tax returns, and who is eligible for sick-exit benefits or public assist programs. The family is divers biologically, legally, or as a social network with personally synthetic ties and ideologies. For some patients family includes just persons related by marriage, birth, or adoption. To others, aunts, uncles, close friends, cohabitating persons, and even pets are family. Your personal beliefs do non take to exist the same as those of your patient. Understand that families accept many forms and have diverse cultural and ethnic orientations. In improver, no two families are alike. Each has its own strengths, weaknesses, resources, and challenges.
Current Trends and New Family Forms
Family forms are patterns of people considered by family members to be included in the family (Box 10-i). Although all families have some things in common, each family form has unique problems and strengths. Maintain an open mind almost what makes up a family so yous do not overlook potential resource and concerns.
Although the institution of the family remains stiff, the family itself is changing. The "typical" family (ii biological parents and children) is no longer the norm. People are marrying later, women are delaying childbirth, and couples are choosing to accept fewer children or none at all. The number of people living lonely is expanding apace and represents approximately 26% of all households. Divorce rates continue to exist high; it is estimated that 54% of marriages will cease in divorce (U.Southward. Agency of the Census, 2008). A number of divorced adults remarry; the median interval between divorce and remarriage is about 3 years. Remarriage often results in a blended family with a complex prepare of relationships among stepparents, stepchildren, one-half brothers and sisters, and extended family members.
Marital roles are also more complex as families increasingly comprise two wage earners. The bulk of women work outside the habitation, and about 60% of mothers are in the workforce (U.S. Agency of the Census, 2008). Balancing employment and family life creates a variety of challenges in terms of child intendance and household piece of work for both parents. The rest for working parents between child care and household duties is positive when the working parents' chore and life satisfactions remain high (Colina, 2005). There is no proof that maternal employment is dissentious for children (Hill, 2005; Shpancer et al., 2006). However, finding quality child care is a major issue. Managing household tasks is another challenge. Although equal division of labor receives verbal approval, most household tasks remain "women's work." In that location is some show that the father's role is changing. Fathers now participate more fully in mean solar day-to-solar day parenting responsibilities. Twenty-4 percent of children (ages 0 to 4) have their fathers as caretakers whether or not the fathers are employed (U.Due south. Bureau of the Demography, 2008).
The number of single-parent families, which doubled from the 1970s to the 1990s, seems to exist stabilizing. Forty-one percentage of children are living with mothers who have never married; many of these children are a consequence of an adolescent pregnancy. Although mothers head most single-parent families, male parent-merely families are on the rise.
Adolescent pregnancy is an ever-increasing business concern. The majority of adolescent mothers continue to live with their families. A teenage pregnancy has long-term consequences for the mother. For example, adolescent mothers frequently quit loftier school and take inadequate job skills and limited wellness intendance resources. The overwhelming chore of existence a parent while still being a teenager often severely stresses family unit relationships and resources. In addition, in that location is an increased risk for subsequent adolescent pregnancy, disability to obtain quality task skills, and poor lifestyles (Harper et al., 2010). Stressors are besides placed on teenage fathers when their partner becomes pregnant. These immature men have poorer back up systems and fewer resources to teach them how to parent. In improver, adolescent fathers report early agin family relationships such as exposure to domestic violence and parental separation or divorce and lack positive fathering function models (Biello, Sipsma, and Kershaw, 2010). As a issue, both adolescent parents often struggle with the normal tasks of development and identity but must take a parenting role that they are non prepare for physically, emotionally, socially, and/or financially.
Many homosexual couples define their relationship in family terms. Approximately half of all gay male couples live together compared with three fourths of lesbian couples. These couples are more open about their sexual preferences and more vocal nigh their legal rights. Some homosexual families include children, either through adoption or artificial insemination or from prior relationships.
The fastest-growing age-group in America is 65 years of age and over. For the first time in history the average American has more than living parents than children, and children are more likely to have living grandparents and even great-grandparents. This "graying" of America continues to affect the family life cycle, particularly the "sandwich generation"—made up of the children of older adults (encounter section on restorative care). These individuals, who are ordinarily in the middle years, have to meet their own needs along with those of their children and their aging parents. This balance of needs oft occurs at the expense of their own well-being and resources. In addition, many of the family caregivers report that support from professional health professionals is lacking (Touhy and Jett, 2010). Most family unit caregivers are women; the boilerplate age is 46, with xiii% existence 65 years of age or older, and they frequently provide more than than 20 hours of intendance per week (Schumacher, Beck, and Marren, 2006a). Caring for a frail or chronically ill relative is a primary business concern for a growing number of families. It is not uncommon for people in their 60s and 70s to exist the major caregivers for i another. Box 10-ii provides a list of family nursing gerontological concerns.
More grandparents are raising their grandchildren (U.S. Agency of the Census, 2008). This new parenting responsibility is the result of a number of societal factors: the increase in the divorce charge per unit, dual-income families, and single parenthood. Most often information technology is a upshot of legal intervention when parents are unfit or renounce their parental obligations.
Families face many challenges, including changing structures and roles in the changing economic status of society. In addition, social scientists identify four further trends as threats or concerns facing the family: (1) changing economical status (eastward.chiliad., declining family income and lack of access to health intendance), (ii) homelessness, (3) family violence, and (iv) the presence of acute or chronic illnesses.
Changing Economic Status
Making ends come across is a daily business organisation considering of the failing economic condition of families. Although two-income families have go the norm, existent family unit income has non increased since 1973. Families at the lower end of the income calibration have been specially affected, and single-parent families are especially vulnerable. Because of recent economic trends adult children are oftentimes faced with moving back dwelling house afterward college considering they cannot discover employment or in some cases lose their jobs.
The number of American children living below the poverty level continues to ascension. The number of children living beneath poverty increased by two one thousand thousand since 2000, and eight.1 million children are uninsured (Children'due south Defense Fund [CDF], 2010). A majority of uninsured children have at least i parent who works simply is unable to afford insurance. When caring for these families, the nurse needs to be sensitive to their desire for independence but as well help them with obtaining appropriate financial and wellness care resources. For case, you inform the family where to get within the community to obtain assist with energy bills, dental and health care, and help with school supplies.
Homelessness
Homelessness is a major public health issue. Co-ordinate to public health organizations, absolute homelessness describes people without concrete shelter who sleep outdoors, in vehicles, in abandoned buildings, or in other places not intended for homo habitation. Relative homelessness describes those who have a physical shelter, but one that does not see the standards of health and safety (National Coalition for the Homeless, 2010).
The fastest growing section of the homeless population is families with children. This includes complete nuclear families and unmarried-parent families. Information technology is expected that 3.5 million people are homeless and 1.35 one thousand thousand are families with children. Poverty, mental and concrete illness, and lack of affordable housing are chief causes of homelessness (National Coalition for the Homeless, 2010). Homelessness severely affects the functioning, health, and well-existence of the family and its members. Children of homeless families are often in off-white or poor health and have higher rates of asthma, ear infections, stomach issues, and mental illness (run across Affiliate iii). As a result, usually the only access to health care for these children is through an emergency department.
Children who are homeless face difficulties such equally coming together residency requirements for public schools, disability to obtain previous enrollment records, and enrolling in and attending schoolhouse. Equally a result, they are more likely to drib out of schoolhouse and get unemployable (National Coalition for the Homeless, 2010). Homeless families and their children are at serious chance for developing long-term health, psychological, and socioeconomic issues. For example, the children are oft underimmunized and at risk for childhood illnesses; they may autumn behind in school and are at take chances of dropping out; or they can develop risky behaviors.
Family unit Violence
The statistics regarding family violence are even more disturbing. Approximately 3.3 to x million children reported existence abused or neglected in the menstruation from 1991 to 2004 (Family unit Violence Prevention Fund, 2008a). Emotional, concrete, and sexual abuse occurs toward spouses, children, and older adults and across all social classes. Factors associated with family violence are complex and include stress, poverty, social isolation, psychopathology, and learned family behavior. Other factors such as alcohol and drug abuse, pregnancy, sexual orientation, and mental disease increase the incidence of abuse within a family (Family unit Violence Prevention Fund, 2008b). Although corruption sometimes ends when one leaves a specific family environment, negative long-term physical and emotional consequences are frequently evident. One of the consequences includes moving from 1 calumniating state of affairs to some other. For example, an adolescent girl sees wedlock as a way to leave her parents' calumniating abode and in plow marries a person who continues the abuse in her marriage.
Acute or Chronic Illness
Any acute or chronic illness influences the entire family economically, emotionally, socially, and functionally and affects the family's decision-making and coping resource. Hospitalization of a family unit fellow member is stressful for the whole family. Hospital environments are foreign, physicians and nurses are strangers, the medical linguistic communication is difficult to understand or interpret, and family unit members are separated from 1 another.
During an acute illness such as a trauma, myocardial infarction, or surgery, family members are oftentimes left in waiting rooms to anticipate data about their loved one. Communication amidst family members may exist misdirected from fearfulness and worry. Sometimes previous family conflicts rise to the surface, whereas others are suppressed. When implementing a patient-centered care model, patients' family members and surrogate decision makers must become active partners in conclusion making and care (Davidson, 2009). Understand the family'due south cultural beliefs and values and demand for communication and back up.
Chronic illnesses are a global health problem. Adaptations to chronic illnesses pose unique challenges for the family unit (Weinert et al., 2008). Ofttimes family patterns and interactions, social activities, piece of work and household schedules, economic resources, and other family unit needs and functions must be reorganized around the chronic disease or disability. Despite the stressors, families also learn how to manage many aspects of their loved one's illness or disability. Astute nursing intendance helps the family prevent and/or manage medical crises, control symptoms, acquire how to provide specific therapies, arrange to changes over the course of the illness, avert isolation, obtain community resource, and assistance in helping the family resolve conflict.
Chronic illnesses are common in a bulk of family unit units. Chronic illness impacts a family unit's quality of life. Families must work at developing working partnerships with the wellness intendance commitment system to place available wellness care and customs resources for illness direction (Weinert et al., 2008). The chronic disease continuum ranges from newly diagnosed illness to finish stages of the disease. The patient'due south level of independence changes over time, and family members demand to accommodate to irresolute caregiving needs (Tamayo et al., 2010). Common chronic illnesses include merely are non limited to asthma, diabetes, cardiovascular illnesses, renal disease, human immunodeficiency virus (HIV), and cancer.
Trauma
Trauma is a sudden unplanned result. Family unit members oftentimes struggle to cope with the challenges of a severe, life-threatening event, which tin include the stressors associated with a family unit member hospitalized in an intensive care environment, loss of a family member, or an astute psychiatric illness. The powerlessness that family members experience makes them very vulnerable and less able to make important decisions most the health of the family. In caring for family members, answer their questions honestly. When y'all exercise non know the respond, find someone who does. Provide realistic balls; giving fake hope breaks the nurse-patient trust and also affects how the family can suit to "bad news." When the victim of trauma is hospitalized, take fourth dimension to make sure that the family is comfy. You can bring them something to eat or potable, give them a blanket, or encourage them to become a meal. Sometimes telling the family that you volition stay with their loved one while they are gone is all they need to feel comfortable in leaving. Most family members have a cell phone and can be reached easily if their loved one's condition changes.
Stop-of-Life Intendance
Y'all will run across many families with a terminally ill member. Although people equate final illness with cancer, many diseases take terminal aspects (east.g., center failure, pulmonary and renal diseases, and neuromuscular diseases). Although some family members may be prepared for their loved one's decease, their need for information, support, assurance, and presence is corking (see Chapter 36). The more than you know about your patient'due south family, how they interact with one another, their strengths, and their weaknesses, the better. Each family approaches and copes with terminate-of-life decisions differently. Requite the family unit information about the dying process. Help the family set up home care if they desire and obtain hospice and other appropriate resources, including grief support. Make certain that the family knows what to practice at the time of decease. If yous are present at the time of expiry, be sensitive to the family'south needs (e.g., provide for privacy and allow sufficient time for saying expert-byes).
Theoretical Approaches: An Overview
A number of different perspectives can be applied when caring for families. It is important that you empathise some of the broader perspectives for family unit nursing. The family wellness system (FHS) and developmental theories are two perspectives used in this chapter to help yous provide nursing intendance to the family as a whole and the individuals within the family structure. These theoretical perspectives and their concepts provide the foundation for family cess and interventions.
Family unit Health Organisation
When assessing the family unit, it is important to use a guide such equally the FHS to identify all of their needs. The FHS is a holistic model that guides the cess and care for families (Anderson, 2000; Anderson and Friedemann, 2010). The FHS includes 5 realms/processes of family life: interactive, developmental, coping, integrity, and health. The FHS approach is one method for family cess to determine areas of concern and strengths, which helps you develop a plan of care with family nursing interventions and outcomes. Every bit with all systems, the FHS has both unspoken and spoken goals, which vary co-ordinate to the stage in the family unit life cycle, family values, and private concerns of the family members. When working with families, the goal of intendance is to ameliorate family wellness or well-existence, help in family direction of illness conditions or transitions, and achieve health outcomes related to the family areas of business.
Developmental Stages
Families, similar individuals, change and grow over time. Although they are far from identical to 1 some other, they tend to go through common stages. Each developmental stage has its own challenges, needs, and resources and includes tasks that need to be completed before the family is able to successfully move on to the adjacent stage. Societal changes and an aging population have caused changes in the stages and transitions in the family life cycle. For example, developed children are not leaving the nest as predictably or as early equally in the past, and many are returning dwelling house. In addition, more people are living into their 80s and 90s. Sixty-five is at present considered the "backside of centre age," and the length of the midlife stage in the family life bicycle has increased, as has the later stage in family unit life.
McGoldrick and Carter based their 1985 archetype model of family life stages on expansion, contraction, and realignment of family relationships that back up the entry, leave, and development of the members (Hanson et al., 2005). This model describes the emotional aspects of lifestyle transition and the changes and tasks necessary for the family to proceed developmentally (Table 10-1). Utilize this model to promote family behaviors to achieve essential tasks and help families prepare for later transitions such equally when helping families gear up for a new babe (come across Chapter 13).
Tabular array 10-1
Stages of the Family unit Life Wheel
| Family Life-Cycle Stage | Emotional Procedure of Transition: Key Principles | Changes in Family unit Condition Required to Proceed Developmentally |
| Unattached young adult | Accepting parent-offspring separation | Differentiation of self in relation to family of origin |
| Development of intimate peer relationships | ||
| Establishment of self in work | ||
| Joining of families through marriage: newly married couple | Committing to new system | Formation of marital system |
| Realignment of relationships with extended families and friends to include spouse | ||
| Family unit with young children | Accepting new generation of members into system | Adjusting marital arrangement to make infinite for children |
| Taking on parental roles | ||
| Realignment of relationships with extended family to include parenting and grandparenting roles | ||
| Family with adolescents | Increasing flexibility of family unit boundaries to include children's independence | Shifting of parent-child relationships to allow adolescents to move into and out of system Refocusing on midlife material and career issues |
| Beginning shift toward concerns for older generation | ||
| Launching children and moving on | Accepting multitude of exits from and entries into family unit system | Adjusting to reduction in family unit size |
| Developing adult-to-adult relationships between grown children and their parents | ||
| Realigning relationships to include in-laws and grandchildren | ||
| Dealing with disabilities and death of parents (grandparents) | ||
| Family in later on life | Accepting shifting of generational roles | Maintaining own or couple operation and interests in the confront of physiological decline; exploring new familial and social role options |
| Making room in system for wisdom and experience of older adults; supporting older generations without overfunctioning for them | ||
| Dealing with retirement | ||
| Dealing with loss of spouse, siblings, and other peers and preparation for own death; a life review, in which i reviews life experiences and decisions |
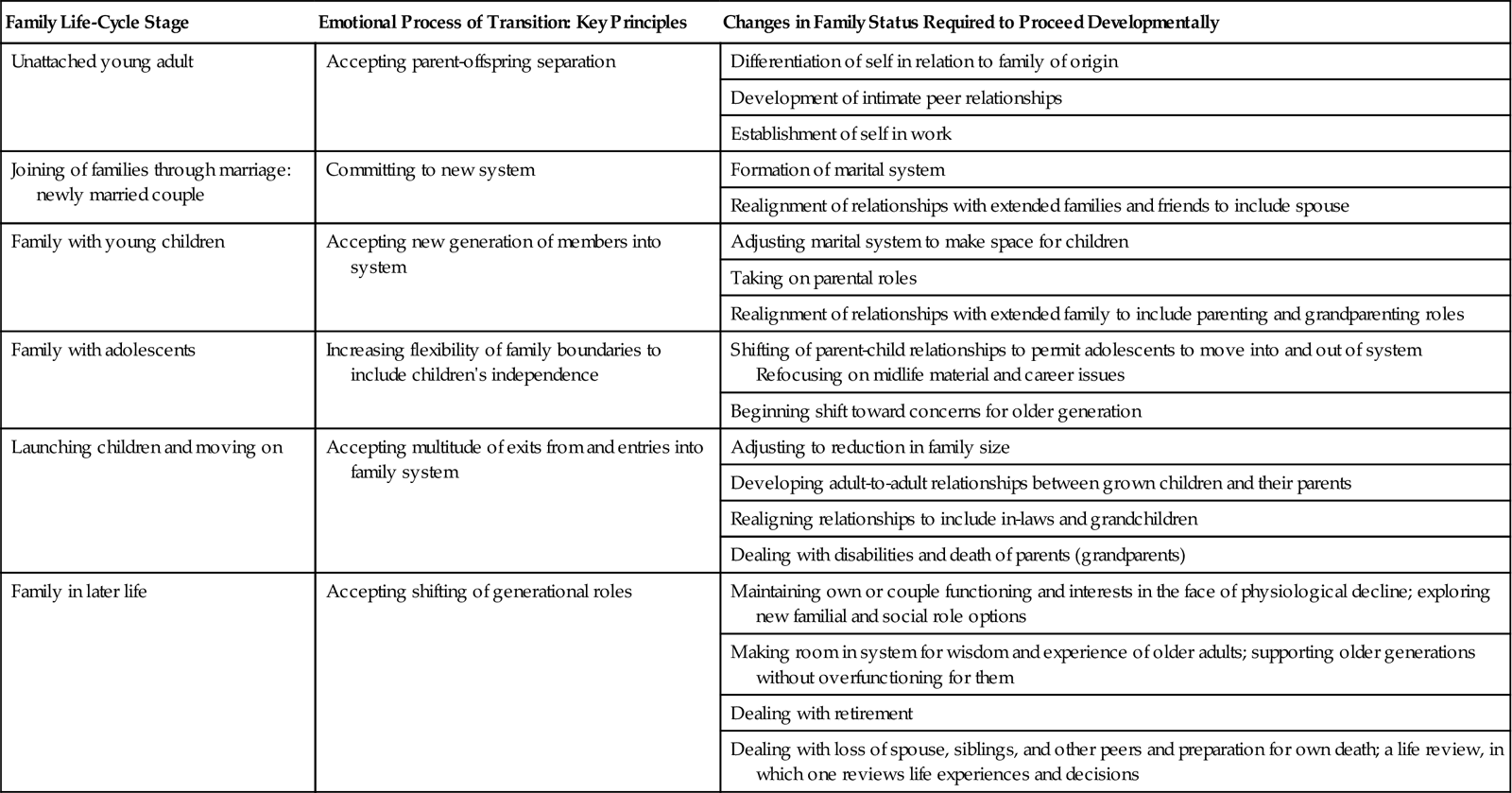
From Duvall EM, Miller BC: Marriage and family development, ed 6, Boston, 2005, Allyn & Bacon. Printed and electronically reproduced by permission of Pearson Education, Inc, Upper Saddle River, NJ.
Attributes of Families
Structure
Families have a construction and a mode of operation. Structure and function are closely related and continually interact with one another. Structure is based on the ongoing membership of the family unit and the pattern of relationships, which are often numerous and complex. For example, a adult female'south relationships frequently include married woman-hubby, female parent-son, mother-daughter, employee-boss, and colleague-colleague, each with unlike demands, roles, and expectations. Patterns of relationships form power and role structures within the family unit. Make up one's mind a family's structures by observing family members' behaviors and interactions.
Structure promotes or impedes the family'south ability to respond to stressors. Very rigid or very flexible structures impair operation. A rigid structure specifically dictates who is able to accomplish a job and may limit the number of persons outside the immediate family who can assume these tasks. For example, in 1 family the mother is the only adequate person to provide emotional support for the children, or the husband is the only one to provide financial back up. A alter in the health condition of the person responsible for a task places a brunt on the family because no other person is available or considered adequate to assume that job. A family must adapt its construction. For example, when a homemaker is ill, the tasks of managing the household (e.g., preparing the meals, maintaining the house, and driving schoolhouse-age children to appointments and events) need to exist shared. The older children may aid set up the meals, and the other parent or a family unit member drives the children to the events, or perhaps the events are rescheduled.
An extremely open structure also presents problems for the family. When the family unit construction is extremely open, consequent patterns of beliefs that lead to automatic action practise non exist. An example is an inconsistent parenting role. The parent sometimes is a strict authoritarian figure and at other times treats the kid as a "best friend and confidant." This type of conduct causes family members to become confused nearly what behavior is appropriate and who is reliable for support. During a crisis or rapid change, family unit members practice not accept a defined structure to "fall back on," and family disintegration is sometimes a result.
Function
Family functioning is what the family does. Specific functional aspects include the way a family reproduces, interacts to socialize its immature, cooperates to encounter economical needs, and relates to the larger society. Family functioning also focuses on the processes used by the family to achieve its goals. Some processes include communication among family members, goal setting, disharmonize resolution, caregiving, nurturing, and use of internal and external resource. Traditional reproductive, sexual, economic, and educational goals that were one time universal family goals no longer apply to all families. For example, a married couple who decides not to have children nevertheless consider themselves a family unit. Another example includes a blended family whose spouses bring schoolhouse-age children into the new marriage. However, the spouses make up one's mind non to co-mingle their finances and have split up educational goals for their pocket-size children. Every bit a result, this family does not accept the traditional economical patterns of a nuclear family.
Families achieve goals more successfully when communication is articulate and direct. Clear communication enhances trouble solving and conflict resolution, and it facilitates coping with life-changing or life-threatening stressors. Some other process to facilitate goal achievement includes the ability to nurture and promote growth. For instance, families might have a specific celebration for a good report carte du jour, a job well done, or specific milestones. They also nurture by helping children know right and wrong. In this situation a family might accept a specific form of discipline such as "time out" or taking abroad privilege, and the children know why the discipline is given. Thus when a situation occurs, the kid is disciplined and learns not to behave like that again.
Families need to have multiple resource bachelor. For case, a social network is an excellent resource. Social relationships such as friends or churches within the community are important for family unit celebrations simply also act as buffers, particularly during times of stress, and reduce a family's vulnerability.
The Family and Health
Many factors influence the wellness of the family (e.grand., its relative position in society, economic resources, and geographical boundaries). Although American families exist within the same culture, they alive in very different ways as a consequence of race, values, social form, and ethnicity. In some minority groups multiple generations of single-parent families live together in one domicile. Grade and ethnicity produce differences in the access of families to the resources and rewards of society. This access creates differences in family life, most significantly in different life chances for its members.
Distribution of wealth greatly affects the capacity to maintain health. Low educational preparation, poverty, and decreased social support compound one another, magnifying their effect on sickness in the family, and magnifying the amount of sickness in the family. Economical stability increases a family'due south access to adequate health care, creates more than opportunity for pedagogy, increases good nutrition, and decreases stress (National Coalition of the Homeless, 2010; Children's Defence force Fund, 2010).
The family is the chief social context in which health promotion and illness prevention have identify. The family's behavior, values, and practices strongly influence health-promoting behaviors of its members (Epley et al., 2010). In turn the health status of each individual influences how the family unit functions and its power to achieve goals. When the family unit satisfactorily functions to meet its goals, its members tend to feel positive about themselves and their family. Conversely, when they do not encounter goals, families view themselves as ineffective.
Some families do not place a high value on skillful health. In fact, some families accept harmful practices. In some cases a family member gives mixed messages about health. For instance, a parent continues to smoke while telling children that smoking is bad for them. Family environment is crucial because health behavior reinforced in early on life has a potent influence on afterwards health practices. In addition, the family environment is a crucial factor in an individual'southward adjustment to a crisis. Although relationships are strained when confronted with illness, research indicates that family members tin have the potential to be a master force for coping (Bluvol and Ford-Gilboe, 2004).
Attributes of Healthy Families
The family is a dynamic unit; it is exposed to threats, strengths, changes, and challenges. Some families are crisis proof, whereas others are crisis decumbent. The crisis-proof, or effective, family is able to combine the demand for stability with the need for growth and change. This type of family has a flexible construction that allows adaptable functioning of tasks and acceptance of help from outside the family unit system. The structure is flexible enough to allow adaptability but not then flexible that the family lacks cohesiveness and a sense of stability. The effective family has command over the environment and influences the immediate environment of dwelling, neighborhood, and schoolhouse. The ineffective, or crisis-prone, family lacks or believes it lacks control over the environments.
Wellness promotion research oft focuses on the stress-moderating effect of hardiness and resiliency as factors that contribute to long-term health. Family unit hardiness is the internal strengths and immovability of the family unit. A sense of command over the event of life, a view of alter as beneficial and growth producing, and an active rather than passive orientation in adapting to stressful events characterize family hardiness (McCubbin, McCubbin, and Thompson, 1996). Family resiliency is the ability to cope with expected and unexpected stressors. Information technology helps to evaluate healthy responses when individuals and families are experiencing stressful events. Resources and techniques that a family or individuals within the family utilise to maintain a balance or level of health assist in agreement a family's level of resiliency.
Family Nursing
To provide compassion and caring for your patients and their families, yous need a scientific knowledge base of operations in family theory and knowledge in family nursing. A focus on the family is necessary to safely belch patients dorsum to the family or community settings. The members of the family unit may need to assume the office of primary caregiver. Family caregivers take unique nursing and caregiving needs and too oft feel abandoned past the health care system (Reinhard, 2006). When a life-irresolute affliction occurs, the family has to make major adjustments to intendance for a family member. Often the psychological, social, and health care needs of the caregiver go unmet (Tamayo et al., 2010).
Family nursing is based on the assumption that all people, regardless of age, are members of some type of family unit form, such every bit the traditional nuclear family or an alternate family. The goal of family nursing is to help the family and its individual members reach and maintain maximum health throughout and beyond the illness experience (Box 10-3). Family nursing is the focus of the future across all practice settings and is of import in all health intendance environments.
Source: https://nursekey.com/caring-for-families/
0 Response to "What Are the Goals of Care When Working With Families According to the Family Health System?"
Post a Comment